General Information About Adrenocortical Carcinoma
Adrenocortical carcinoma is a rare disease in which malignant (cancer) cells form in the outer layer of the adrenal gland.
There are two adrenal glands. The adrenal glands are small and shaped like a triangle. One adrenal gland sits on top of each kidney. Each adrenal gland has two parts. The outer layer of the adrenal gland is the adrenal cortex. The center of the adrenal gland is the adrenal medulla. 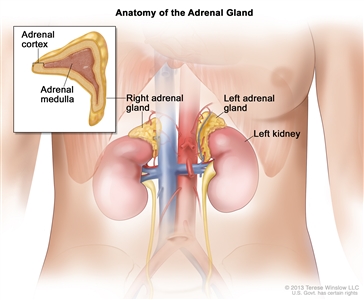
Anatomy of the adrenal gland. There are two adrenal glands, one on top of each kidney. The outer part of each gland is the adrenal cortex and the inner part is the adrenal medulla.
The adrenal cortex makes important hormones that:
- Balance the water and salt in the body.
- Help keep blood pressure normal.
- Help control the body's use of protein, fat, and carbohydrates.
- Cause the body to have masculine or feminine characteristics.
Adrenocortical carcinoma is also called cancer of the adrenal cortex. A tumor of the adrenal cortex may be functioning (makes more hormones than normal) or nonfunctioning (does not make more hormones than normal). Most adrenocortical tumors are functioning. The hormones made by functioning tumors may cause certain signs or symptoms of disease.
The adrenal medulla makes hormones that help the body react to stress. Cancer that forms in the adrenal medulla is called pheochromocytoma and is not discussed in this summary. For more information, see Pheochromocytoma and Paraganglioma.
Adrenocortical carcinoma and pheochromocytoma can occur in both adults and children. Treatment for children, however, is different than treatment for adults. For more information, see Childhood Adrenocortical Carcinoma Treatment and Childhood Pheochromocytoma and Paraganglioma Treatment.
Having certain genetic conditions increases the risk of adrenocortical carcinoma.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your doctor if you think you may be at risk.
Risk factors for adrenocortical carcinoma include having the following hereditary diseases:
- Li-Fraumeni syndrome.
- Beckwith-Wiedemann syndrome.
- Carney complex.
Symptoms of adrenocortical carcinoma include pain in the abdomen.
These and other signs and symptoms may be caused by adrenocortical carcinoma:
- A lump in the abdomen.
- Pain the abdomen or back.
- A feeling of fullness in the abdomen.
A nonfunctioning adrenocortical tumor may not cause signs or symptoms in the early stages.
A functioning adrenocortical tumor makes too much of one of the following hormones:
- Cortisol.
- Aldosterone.
- Testosterone.
- Estrogen.
Too much cortisol may cause:
- Weight gain in the face, neck, and trunk of the body and thin arms and legs.
- Growth of fine hair on the face, upper back, or arms.
- A round, red, full face.
- A lump of fat on the back of the neck.
- A deepening of the voice and swelling of the sex organs or breasts in both males and females.
- Muscle weakness.
- High blood sugar.
- High blood pressure.
Too much aldosterone may cause:
- High blood pressure.
- Muscle weakness or cramps.
- Frequent urination.
- Feeling thirsty.
Too much testosterone (in women) may cause:
- Growth of fine hair on the face, upper back, or arms.
- Acne.
- Balding.
- A deepening of the voice.
- No menstrual periods.
Men who make too much testosterone do not usually have signs or symptoms.
Too much estrogen (in women) may cause:
- Irregular menstrual periods in women who have not gone through menopause.
- Vaginal bleeding in women who have gone through menopause.
- Weight gain.
Too much estrogen (in men) may cause:
- Growth of breast tissue.
- Lower sex drive.
- Impotence.
These and other signs and symptoms may be caused by adrenocortical carcinoma or by other conditions. Check with your doctor if you have any of these problems.
Imaging studies and tests that examine the blood and urine are used to diagnose adrenocortical carcinoma.
The tests and procedures used to diagnose adrenocortical carcinoma depend on the patient's signs and symptoms. The following tests and procedures may be used:
-
Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
-
Twenty-four-hour urine test: A test in which urine is collected for 24 hours to measure the amounts of cortisol or 17-ketosteroids. A higher than normal amount of these in the urine may be a sign of disease in the adrenal cortex.
-
Low-dose dexamethasone suppression test: A test in which one or more small doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol.
-
High-dose dexamethasone suppression test: A test in which one or more high doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol or if the pituitary gland is telling the adrenal glands to make too much cortisol.
-
Blood chemistry study: A procedure in which a blood sample is checked to measure the amounts of certain substances, such as potassium or sodium, released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
-
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
-
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI). An MRI of the abdomen is done to diagnose adrenocortical carcinoma.
-
Adrenal angiography: A procedure to look at the arteries and the flow of blood near the adrenal glands. A contrast dye is injected into the adrenal arteries. As the dye moves through the arteries, a series of x-rays are taken to see if any arteries are blocked.
-
Adrenal venography: A procedure to look at the adrenal veins and the flow of blood near the adrenal glands. A contrast dye is injected into an adrenal vein. As the contrast dye moves through the veins, a series of x-rays are taken to see if any veins are blocked. A catheter (very thin tube) may be inserted into the vein to take a blood sample, which is checked for abnormal hormone levels.
-
PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
-
MIBG scan: A very small amount of radioactive material called MIBG is injected into a vein and travels through the bloodstream. Adrenal gland cells take up the radioactive material and are detected by a device that measures radiation. This scan is done to tell the difference between adrenocortical carcinoma and pheochromocytoma.
-
Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The sample may be taken using a thin needle, called a fine-needle aspiration (FNA) biopsy or a wider needle, called a core biopsy.
Certain factors affect the prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- The stage of the cancer (the size of the tumor and whether it is in the adrenal gland only or has spread to other places in the body).
- Whether the tumor can be completely removed in surgery.
- Whether the cancer has been treated in the past.
- The patient's general health.
- The grade of tumor cells (how different they look from normal cells under a microscope).
Adrenocortical carcinoma may be cured if treated at an early stage.
Stages of Adrenocortical Carcinoma
After adrenocortical carcinoma has been diagnosed, tests are done to find out if cancer cells have spread within the adrenal gland or to other parts of the body.
The process used to find out if cancer has spread within the adrenal gland or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following tests and procedures may be used in the staging process:
-
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the abdomen or chest, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
-
MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the abdomen. A substance called gadolinium may be injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
-
PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
-
Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs, such as the vena cava, and make echoes. The echoes form a picture of body tissues called a sonogram.
-
Adrenalectomy: A procedure to remove the affected adrenal gland. A tissue sample is viewed under a microscope by a pathologist to check for signs of cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if adrenocortical carcinoma spreads to the lung, the cancer cells in the lung are actually adrenocortical carcinoma cells. The disease is metastatic adrenocortical carcinoma, not lung cancer.
The following stages are used for adrenocortical carcinoma:
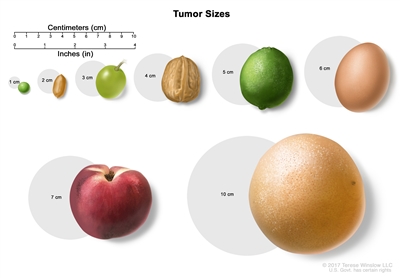
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage I
In stage I, the tumor is 5 centimeters or smaller and is found in the adrenal gland only.
Stage II
In stage II, the tumor is larger than 5 centimeters and is found in the adrenal gland only.
Stage III
In stage III, the tumor is any size and has spread:
- to nearby lymph nodes; or
- to nearby tissues or organs (kidney, diaphragm, pancreas, spleen, or liver) or to large blood vessels (renal vein or vena cava) and may have spread to nearby lymph nodes.
Stage IV
In stage IV, the tumor is any size, may have spread to nearby lymph nodes, and has spread to other parts of the body, such as the lung, bone, or peritoneum.
Adrenocortical carcinoma can recur (come back) after it has been treated.
The cancer may come back in the adrenal cortex or in other parts of the body.
Treatment Option Overview
There are different types of treatment for patients with adrenocortical carcinoma.
Different types of treatments are available for patients with adrenocortical carcinoma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
The following types of treatment are used:
Surgery
Surgery to remove the adrenal gland (adrenalectomy) is often used to treat adrenocortical carcinoma. Sometimes surgery is done to remove the nearby lymph nodes and other tissue where the cancer has spread.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is treatment using more than one anticancer drug. The way the chemotherapy is given depends on the type and stage of the cancer being treated.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Immunotherapy
Immunotherapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This cancer treatment is a type of biologic therapy.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells.
Treatment for adrenocortical carcinoma may cause side effects.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Treatment of Stage I Adrenocortical Carcinoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of stage I adrenocortical carcinoma may include the following:
- Surgery (adrenalectomy). Nearby lymph nodes may also be removed if they are larger than normal.
- A clinical trial of a new treatment.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage II Adrenocortical Carcinoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of stage II adrenocortical carcinoma may include the following:
- Surgery (adrenalectomy). Nearby lymph nodes may also be removed if they are larger than normal.
- A clinical trial of a new treatment.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage III Adrenocortical Carcinoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of stage III adrenocortical carcinoma may include the following:
- Surgery (adrenalectomy). Nearby lymph nodes may also be removed if they are larger than normal.
- A clinical trial of radiation therapy.
- A clinical trial of a new treatment.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage IV Adrenocortical Carcinoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of stage IV adrenocortical carcinoma may include the following as palliative therapy to relieve symptoms and improve the quality of life:
- Chemotherapy or combination chemotherapy.
- Radiation therapy to bones or other sites where cancer has spread.
- Surgery to remove cancer that has spread to tissues near the adrenal cortex.
- A clinical trial of chemotherapy, immunotherapy, or targeted therapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Recurrent Adrenocortical Carcinoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of recurrent adrenocortical carcinoma may include the following as palliative therapy to relieve symptoms and improve the quality of life:
- Surgery.
- Radiation therapy.
- A clinical trial of chemotherapy or immunotherapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Adrenocortical Carcinoma
For more information from the National Cancer Institute about adrenocortical carcinoma, see the following:
For general cancer information and other resources from the National Cancer Institute, visit:
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of adult adrenocortical carcinoma. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Adrenocortical Carcinoma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/adrenocortical/patient/adrenocortical-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389225]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2023-02-15
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.


